MEchanical Ventilation
Scalars
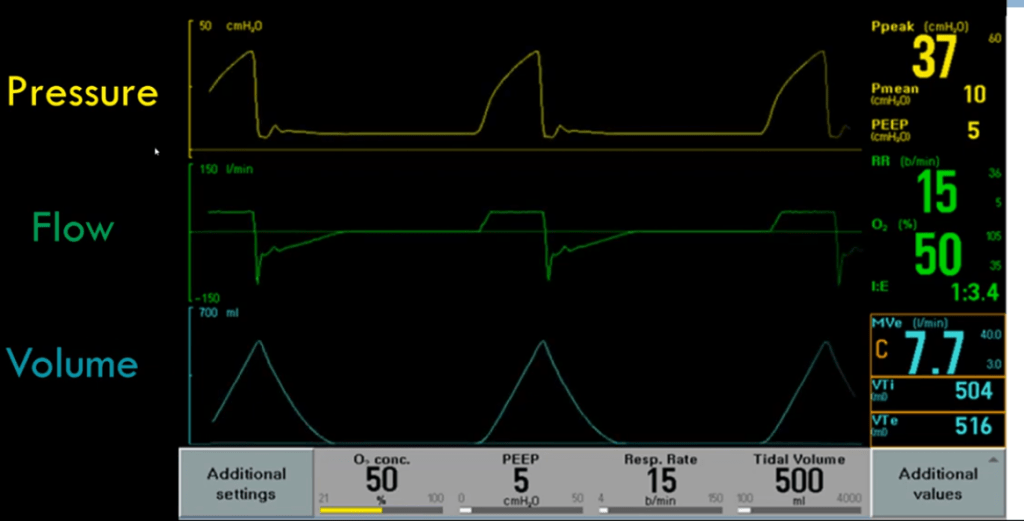
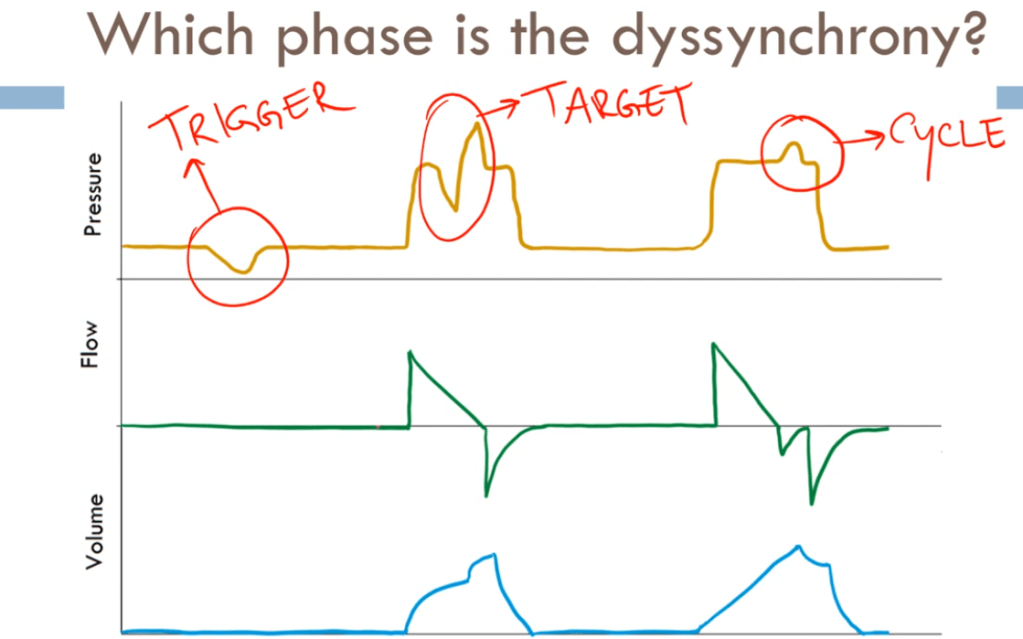
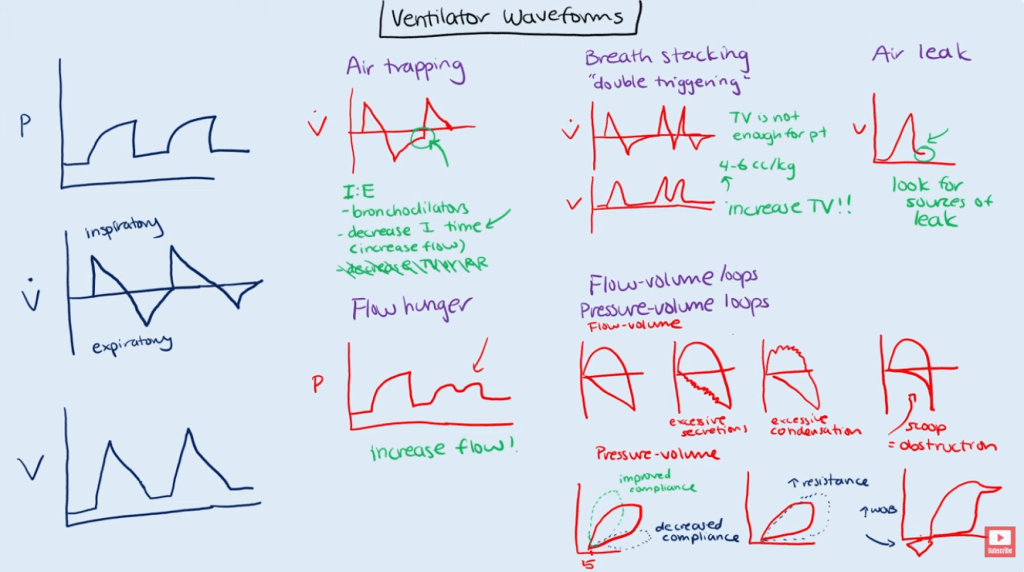
Ventilators commonly display three scalars:
- Pressure–time scalar (pressure waveform)
- Flow–time scalar (flow waveform)
- Volume–time scalar (volume waveform)
Ventilator Waveforms trouble shooting
Air trapping
Major Ventilator Troubleshooting: High-Yield Summary
1. Air Trapping (Auto-PEEP)
Where to look
- Flow–time waveform
- Expiratory flow does not return to baseline before the next breath
Who gets it
- COPD, asthma, emphysema
- Obstructive physiology
Core problem
- Inadequate expiratory time → trapped air
Fix (key principle: ↑ expiratory time)
- ↓ Inspiratory time
- Pressure control: shorten Ti
- Volume control: ↑ inspiratory flow
- ↓ Respiratory rate (if needed)
- ↓ Tidal volume (last resort)
- Give bronchodilators
- Avoid unnecessary increases in minute ventilation
2. Breath Stacking / Double Triggering
Where to look
- Flow waveform: two inspirations back-to-back
- Volume waveform: double volume spikes in quick succession
What it means
- Patient’s inspiratory demand > delivered tidal volume
- Common during low tidal volume ventilation
Why it matters
- ↑ Risk of volutrauma and barotrauma
Fix
- Increase tidal volume (within safe limits)
- Consider adjusting inspiratory time or mode
- Improve patient comfort/synchrony (analgesia, sedation if needed)
3. Air Leak
Where to look
- Volume–time waveform
- Inspired and expired volumes do not match (volume doesn’t return to baseline)
First step
- Check flow waveform
- If flow doesn’t return to baseline → air trapping
- If flow does return → true leak
Common causes
- Endotracheal tube cuff leak
- Circuit disconnection
- Bronchopleural fistula
- Pneumothorax
Fix
- Check cuff pressure
- Inspect circuit
- Evaluate patient (lung exam, CXR)
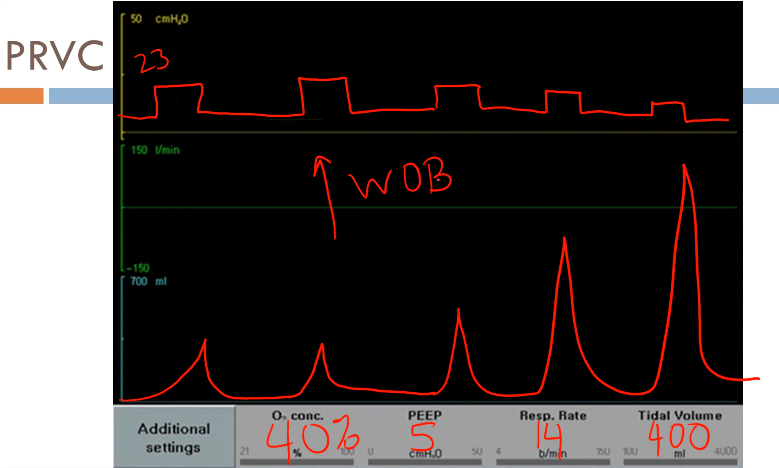
4. Flow Hunger
Where to look
- Pressure–time waveform
- “Camel hump” or scooped pressure curve instead of smooth plateau
What it means
- Patient wants more inspiratory flow
Fix
- Increase inspiratory flow
- Adjust rise time
- Consider switching to pressure control if appropriate
5. Flow–Volume Loop Abnormalities
Normal
- Smooth inspiratory and expiratory limbs
Abnormal patterns
- Jagged / saw-tooth → excessive secretions
- Inspiratory irregularities → condensation in tubing
- Scooped expiratory limb → obstructive lung disease (COPD/asthma)
Fix
- Suction secretions
- Drain tubing condensation
- Treat obstruction (bronchodilators, steroids)
6. Pressure–Volume Loop Abnormalities
What PV loops tell you
- Compliance
- Resistance
- Work of breathing
- Overdistension
Patterns
- More upright loop → improved compliance
- Flatter loop → worsening compliance
- Wider loop → increased airway resistance
Danger signs
- Fishtail appearance
- Increased work of breathing
- Trigger too insensitive
→ Fix trigger sensitivity
- Bird-beak appearance
- Alveolar overdistension
→ ↓ PEEP, ↓ driving pressure, ↓ tidal volume
- Alveolar overdistension
One-Line Mental Checklist (ICU-Ready)
Flow not back to baseline? → Air trapping
Two breaths in a row? → Increase VT
Volume mismatch? → Leak vs air trapping
Camel hump pressure? → Increase flow
Bird-beak PV loop? → Overdistension

Leave a comment